The following
examples illustrate some of the issues
which have arisen during discussion and
training sessions, specifically relating
to normal, static, slow and excessive growth.
Example 1 - Normal Growth
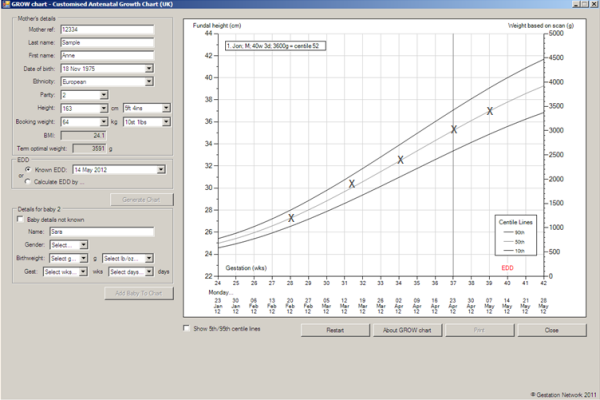
Normal variability in measurement means
that the slope will alter from one measurement
to another. The line may cross centiles,
but the overall slope of the curve should
not be static (no growth over 2-3 weeks)
and becomes abnormal if the slope falls
away in subsequent measurements. In the
case of normal fundal height growth,
the measurements should reflect the curve
on the customised charts. Using these
charts in very small and very large women
should reduce the number who will be
referred for ultrasound assessment.
Example 2 – Static Growth
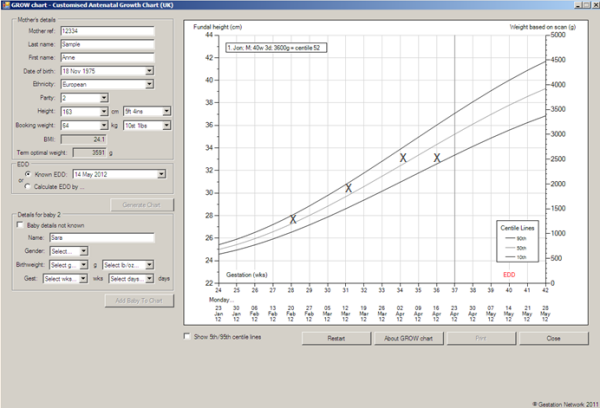
In this example, the measurement is identical
in two measurements separated by 2 weeks.
We would consider this to be an abnormal
pattern, and should prompt referral for
ultrasound assessment. Static growth has
the same significance whether the original
measurement is above the 90th Centile,
on the 50th, or on the 10th Centile. The
potential impaction is static fetal growth,
and possibly also reduced liquor volume,
both of which are associated with intrauterine
death.
Example 3 – Slow Growth
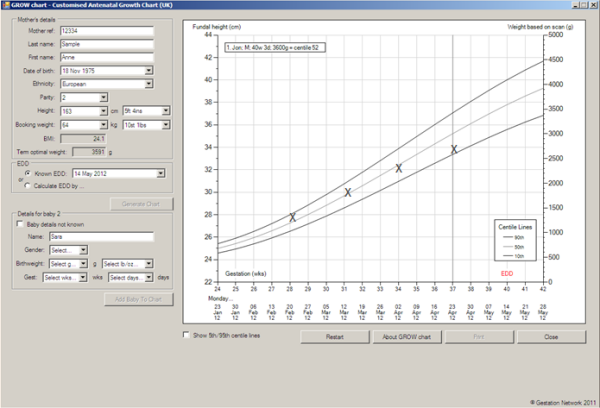
It might be difficult to determine when
then growth of the fundal height is slow.
The essential feature is that you are concerned
about it, and it is likely that the pattern
will have emerged over 3 or 4 measurements.
We are not able to define the referral
criteria, but growth curves which cross
centiles from higher to lower are of concern.
It is absolutely vital that you plot your
fundal height measurements correctly with
a cross, so that the radiographer or midwife
undertaking the ultrasound assessment can
see clearly why you have referred the case.
If the EFW is similarly clearly plotted
(with an open circle) you will have the
ultrasound assessment of fetal weight,
put into context by the customised chart.
Example
4 – Excessive Growth
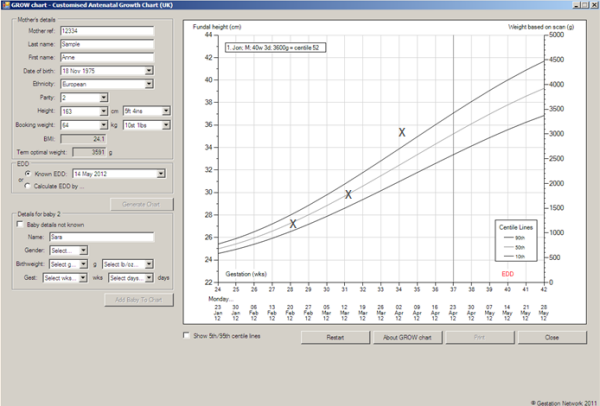
The clinical concerns about large for
dates are very much less than small for
dates. A large for dates pregnancy might
be first presentation of gestational diabetes,
which can present with both a large baby
and polyhydramnios. The ultrasound assessment
will address the issue of fetal size and
polyhydramnios, and should prompt a re-evaluation
of the fetus for structural anomalies.
Large babies can be very difficult to predict
using Ultrasound, and it is even more difficult
to know whether to recommend elective caesarean
sections in these cases. The evidence to
date is that the diagnosis of macrosomia
in the fetus is of doubtful benefit in
terms of improving the outcome, once of
the issues of diabetes have been resolved.
The fundal height measurement is known
to have considerable variability, often
being above the 90th Centile on the customised
charts in the 24 – 30 week range.
We therefore recommend that an initial
measurement above the 90th Centile does
not prompt ultrasound referral, but is
repeated and is only assessed by ultrasound
examination if the plot increases steeply
(which might occur with polyhydramnios).
The emphasis here is again on using your
clinical judgement, if the circumstances
are those where there is a high risk of
gestational diabetes, the expectant mother
will be offered screening for diabetes
with a random blood sugar or GTT.
Cases showing a large fundal height will
contain some interesting cases with rare
complications of pregnancy, but we must
remember that the initial observations
at 24- 28 weeks are very frequently above
the 90th Centile, because the customised
charts have been produced with the estimated
fetal weight primarily in line.
Good communication is essential, and one
message, which can be quite frightening
to a mother, is that she is having a big
baby. It is therefore appropriate to reassure
the mother and repeat the fundal height
measurement 2 to 3 weeks later. Ultrasound
is notoriously poor at predicting the weight
of big babies, a calming reassuring approach
is very important.
|

