INTRODUCTION
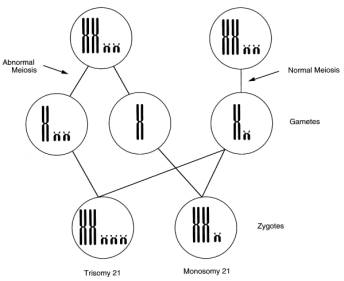
| Down's Syndrome is caused by an additional
copy of chromosome 21 and is the most common
condition associated with autosomal aneuploidy
at birth. The majority of Down's Syndrome conceptions
are lost through spontaneous miscarriage, mainly
very early on, but with decreasing frequency
throughout pregnancy. |
 |
Down's Syndrome is an important cause
of structural anomalies and it is the biggest single
cause of learning difficulties.
The vast majority of cases of Down's Syndrome are due to non-disjunction (a
failure of the normal separation of a pair of chromosomes during cell division).
Trisomy 21, as well as other autosomal trisomies, is more common with increasing
maternal age .
Top of Page
ANTENATAL
Biochemical screening for Down's Syndrome was developed
during the 1980's. The principle of this method is
to refine the risk for an individual by measuring
pregnancy related hormones and proteins, which are
present in different quantities in a population of
trisomy 21 pregnancies, compared with unaffected
ones. Biochemical screening has traditionally been
undertaken at 16 to 18 weeks of pregnancy. Measuring
the levels of serum hormones and comparing them to
median values for the same gestation allows a multiple
of the median (MoM) to be calculated. The risk can
be further refined by standardising for maternal
weight and ethnic group.
Ultrasound is increasingly used to examine the
fetus for structural anomalies. Ultrasound screening
is often undertaken at 18 to 22 weeks gestation,
with the express purpose of identifying structural
congenital anomalies. Some specific diagnoses are
commonly associated with trisomy 21; these include
atrioventricular septal defects, Fallot's tetralogy,
exomphalos, hydrocephalus, duodenal atresia and diaphragmatic
hernia. These conditions, where there is a high chance
of fetal trisomy, are known as "hard markers".
The other circumstance where ultrasound can raise
suspicion of trisomy is when a number of sonographic "soft
markers" are seen. These are not, in the real
sense, congenital anomalies, and if they are not
associated with trisomy, there is no known adverse
outcome for the pregnancy. These include brachycephaly,
nuchal pad, choroid plexus cysts, echogenic foci
in the heart, echogenic bowel, mildly dilated renal
pelvis, short femur, sandal gap, clinodactyly, and
hypoplastic middle phalanx of little finger. Some
of these findings may raise concerns other than trisomy,
but a combination of these soft markers in a fetus
is associated with an increasing risk of trisomy.
Screening for trisomy 21 using nuchal translucency
measurements by ultrasound is a relatively recent
development. The principle is the same as for serum
screening but is undertaken at 10 to 14 weeks. A
measurement is taken of the sonolucent layer within
the skin at the back of the fetal neck and compared
with a median value for that gestation. The age-related
risk is then adjusted up or down to give an individual
risk for that pregnancy.
Top of Page
POSTNATAL
A main concern for parents is the fact that people
with Down's Syndrome have moderate to severe learning
difficulties. Other congenital malformations are
common in babies with Down's Syndrome, particularly
congenital heart disease (including atrioventricular
septal defect, common atrioventricular canal and
patent ductus arteriosus), but also duodenal atresia.
Other common findings include short stature and squint.
Survival in Down's Syndrome has improved considerably
over the years, particularly with improvements in
the correction of congenital heart defects. Overall,
85% of infants now survive to one year, compared
with 70% of those with congenital heart disease.
More than 50% now live beyond 50 years. Other deaths
are mainly due to other congenital malformations
and respiratory infections.
Top of Page
WEST MIDLANDS
DATA
Top of Page

